Diaton Tonometer and Corneal-Independent IOP Screening in Glaucoma Care
Glaucoma screening still depends heavily on one clinical variable: intraocular pressure (IOP). But while IOP is central to glaucoma detection and monitoring, the way it is measured can be influenced by the very tissue most traditional tonometers depend on — the cornea.
That matters more today than it did a generation ago.
Modern eye care is filled with patients whose corneas no longer fit the assumptions built into legacy tonometry. Refractive surgery, age-related tissue change, corneal thinning, keratoconus, scarring, edema, and variations in corneal biomechanics can all complicate the interpretation of corneal-based IOP readings. In these patients, clinicians may benefit from an additional perspective — one that bypasses the cornea altogether.
The Diaton® transpalpebral tonometer was designed for exactly that purpose. By measuring IOP through the upper eyelid over the sclera, it provides a corneal-independent screening pathway that can complement traditional tonometry in modern glaucoma care.
This article explains why corneal-independent IOP screening matters, how the Diaton measurement system works, and where it may add value in real-world clinical workflows.
The Problem with a Cornea-Dependent Reading in a Cornea-Variable World
Goldmann applanation tonometry remains the historical reference point in glaucoma care, and its role is deeply established. But like other corneal tonometers, Goldmann derives its reading from the cornea itself. That means the final number is not purely about intraocular pressure; it is also influenced by the mechanical behavior of the corneal tissue being measured.
Among the corneal variables that can affect interpretation are:
- central corneal thickness (CCT)
- corneal hysteresis
- rigidity or elasticity
- post-surgical biomechanical change
- surface irregularity, scarring, or edema
In some patients, those variables are relatively modest. In others, they are central to the case.
Post-LASIK and post-refractive patients
Refractive procedures such as LASIK, PRK, and SMILE alter the structure of the cornea permanently. As a result, corneal applanation readings in these eyes may not behave the same way they do in untouched corneas. That does not make corneal tonometry unusable — but it does make context and interpretation more important.
Thin or structurally atypical corneas
Keratoconus, corneal thinning, post-surgical change, scarring, and edema can all alter the mechanical properties of the tissue being measured. In these cases, an IOP value obtained through the cornea may reflect both pressure and corneal biomechanics.
This is where a corneal-independent pathway becomes clinically useful.
What Makes the Diaton Tonometer Different
The Diaton tonometer does not applanate the cornea and does not measure through it. Instead, it performs a transpalpebral measurement through the upper eyelid over the sclera.
That distinction is more than a technical curiosity. It changes the measurement pathway entirely.
By bypassing the cornea, Diaton avoids the need to interpret the reading through the lens of corneal thickness, corneal rigidity, or post-refractive corneal change. The result is not a replacement for all other tonometry — it is a different measurement route, and in many cases, a very useful one.
This is why Diaton is best viewed as a complementary screening tool in glaucoma care, particularly for patients whose corneas are less predictable than the textbook ideal.
A Mechanical Measurement System Built Around Fixed Inputs
At the center of the Diaton device is a ballistic transpalpebral measurement mechanism based on classical mechanics.
A small internal component — commonly referred to as the floater — travels through a short, controlled free-fall path inside the instrument. When released, it contacts the eyelid overlying the sclera and rebounds. The Diaton then evaluates the characteristics of that rebound.
Unlike corneal applanation, the system does not infer pressure by flattening the cornea. Instead, it uses a mechanically controlled interaction with the eyelid/scleral interface.
Three core elements of the system are fixed by design:
1. A fixed floater mass
The internal rod is manufactured to a precise weight specification.
2. A fixed drop distance
The path through which the floater travels is mechanically defined during production.
3. A gravity-driven fall
The device depends on a controlled vertical free-fall when positioned properly.
These fixed inputs are important because they make the device’s internal measurement process mechanically stable and repeatable by design. In practical terms, when readings vary, the cause is more likely to be found in patient positioning, lid handling, alignment, or tissue contact than in the core measurement mechanism itself.
Why the Diaton Technique Looks Different from Goldmann Technique
One of the biggest misunderstandings about Diaton comes from assuming it should be used exactly like a corneal tonometer. It should not.
The Diaton is measuring through the eyelid over the sclera, and its internal mechanism depends on gravity. That means the setup and positioning logic are different.
Head position matters
With corneal tonometers such as Goldmann, Tonopen, or iCare, the patient is often upright. Diaton, by contrast, works best when the patient’s head is as horizontal as possible, because the internal floater needs a proper vertical path relative to the eye.
This can be achieved with the patient:
- lying supine, or
- seated and reclined, with the head tilted back into a near-horizontal position
The eye must be directed properly
A common technique is to ask the patient to look at their thumb held at roughly a 45° angle. This helps bring the eye into the correct position and improves access to the intended scleral target zone.
The cornea must be cleared
The upper lid is lifted gently so that the measurement occurs over the tarsal plate and sclera, not the cornea. A useful mental model is to think of the cornea as a “do not touch” zone under an imaginary contact lens edge.
Why Proper Placement Produces Repeatable Readings

Diaton’s consistency comes from the fact that its internal mechanics are fixed. The remaining variable is the anatomical target.
When the device is placed correctly over the tarsal plate and sclera, with minimal lid tension and correct alignment, the system is evaluating the tissue it was designed to measure. That is why the technique is not just “operator preference” — it is part of the measurement pathway itself.
Two common examples help illustrate this:
If the lid is pulled too tightly
Excessive lid tension can make the tissue firmer at the point of contact and may produce a higher reading.
If the contact drifts onto the cornea
Because the cornea is softer than the intended scleral zone, a measurement that slips onto the cornea may produce a lower reading.
These are not random errors. They are predictable consequences of where the device is measuring. Once the user understands that relationship, the technique becomes easier to master and troubleshoot.
How the Device Helps the User Confirm Proper Technique
Diaton does not expect the operator to guess whether a reading is reliable. It provides several forms of real-time feedback:
Verticality signal
The device emits a continuous beep until it reaches the correct 90° vertical position. When alignment is correct, the sound stops.
Tilt warning
If the measurement is taken off-angle, the display shows the letter “L”, indicating that the device was not properly vertical and the reading should be repeated.
Multi-reading confirmation
The Diaton is designed to work with 2–3 readings per eye, and more if needed in variable conditions. When readings are consistent, the device emits a long beep to indicate that a stable cluster has been achieved and the average can be accepted.
This is one of the reasons the device works well in screening workflows: it supports the operator with feedback rather than relying on blind trust in a single click.
Where Corneal-Independent IOP Screening Can Add the Most Value
Diaton is particularly relevant in patient groups and clinical settings where corneal-based readings may be harder to interpret or harder to obtain comfortably.
Patient populations
Diaton can be especially useful in:
- post-LASIK, PRK, and SMILE eyes
- thin or biomechanically atypical corneas
- keratoconus
- corneal scars or edema
- post-corneal surgery patients
- patients sensitive to corneal contact
- patients in whom corneal access is inconvenient or limited
Clinical environments
The device also lends itself to a wide range of settings, including:
- ophthalmology and optometry clinics
- hospital screening programs
- emergency departments
- urgent care
- mobile eye health outreach
- high-volume practices looking to streamline technician workflow
A Practical Tool for Ophthalmic Technicians and Busy Clinics
One of Diaton’s real-world advantages is that it is not limited to physician-only use. With proper onboarding, it can be integrated effectively into technician-driven workflows.
That matters because glaucoma screening is often not bottlenecked by diagnostic theory — it is bottlenecked by workflow. Devices that require extra setup, topical anesthetic, corneal contact, or complex calibration steps can slow down patient flow and create friction for staff.
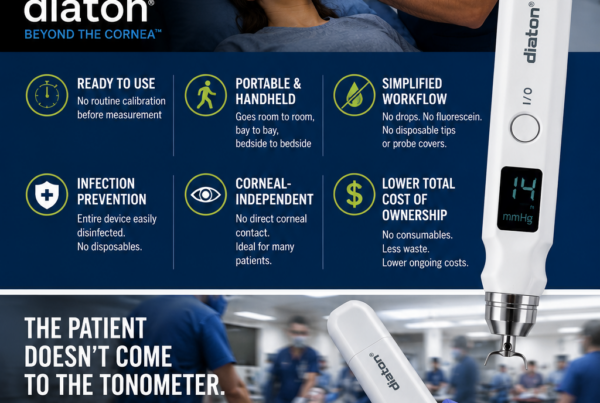
Diaton offers a different workflow profile:
- no corneal contact
- no anesthetic drops
- no disposable tips
- portable handheld design
- clear operator feedback
- quick onboarding for trained staff
For ophthalmic technicians, that can translate into faster workup, simpler screening logistics, and easier adoption in busy clinics.
What the Diaton Is — and What It Is Not
The most useful way to think about the Diaton tonometer is not as a declaration that traditional tonometry is obsolete. It is better understood as an additional measurement perspective.
It is a tool for:
- corneal-independent glaucoma screening
- screening patients with altered corneal biomechanics
- adding another IOP data point when corneal interpretation is less straightforward
- broadening screening access in technician-friendly or portable workflows
It is not a rejection of Goldmann or a claim that corneal tonometry no longer matters. Goldmann remains a foundational part of glaucoma care. Diaton simply expands the clinical toolkit by offering a route to IOP assessment that does not depend on the cornea.
Why This Matters for the Future of Glaucoma Screening
The number of patients with surgically altered, aging, or otherwise non-ideal corneas is not shrinking. At the same time, eye care practices are under growing pressure to screen efficiently, train staff effectively, and make glaucoma detection more accessible across different settings.
That combination makes corneal-independent screening tools increasingly relevant.
The Diaton tonometer sits at the intersection of those needs:
- it offers a through-the-eyelid, scleral measurement pathway
- it avoids corneal contact
- it reduces reliance on corneal biomechanics
- it supports technician-friendly workflows
- and it expands the ways clinicians can approach glaucoma screening in complex eyes
For that reason, Diaton is not best understood as a niche alternative. In the right setting, it is a practical extension of modern glaucoma screening strategy.
Conclusion
Glaucoma screening is evolving because the patients being screened have changed. Corneal surgery, corneal variability, busy clinic workflows, and broader screening needs all challenge the idea that one cornea-dependent method can answer every question equally well.
The Diaton® transpalpebral tonometer offers a useful answer to that challenge. By measuring IOP through the upper eyelid over the sclera, it provides a corneal-independent screening pathway that can complement traditional tonometry in both routine and complex cases.
For clinicians, ophthalmic technicians, hospitals, and screening programs, its value lies in a combination of factors:
- a different measurement route
- a mechanically stable design
- a portable, patient-friendly workflow
- and a way to extend glaucoma screening beyond the limitations of corneal measurement alone
As glaucoma care continues to adapt to modern patient realities, corneal-independent IOP screening deserves a place in the conversation — and Diaton deserves consideration as one of the tools helping move that conversation forward.
Learn more about Diaton Tonometer:
- Diaton product page
- 100 Questions and Answers on Diaton
- How to use the Diaton Tonometer technique
- Diaton in post-LASIK / corneal pathology
- Diaton in emergency medicine / broader screening environments
- Glaucoma screening / glaucoma awareness
Learn more about Diaton Tonometer: www.TonometerDiaton.com
Contact Team Diaton via Phone: 1-877-342-8667